[The following remarks are my condensed version of a train of thought presented by Bret Weinstein and Heather Heying's recent Darkhorse livestream #94. Video posted below.]
We have to ask the question: To what extent are the narratives that we are battling over being fed to us by something that does not have our best collective interest at its core? This does not mean that we’re being fed narratives from somewhere, but that is at least a possibility that would explain in part why this pandemic is being managed so badly.
The two camps being, COVID is not serious, it’s an excuse for authoritarianism. And the other camp being COVID is extremely serious and the authoritarianism isn’t authoritarianism, it’s about doing what’s best for public health.
Both of these are wrong.
It is quite clear that COVID is a very dangerous disease. On the other hand, it does seem to be the excuse for an awful lot of authoritarianism that makes no sense. I suggest there is a litmus test that we can use to detect that there is something about the way this being handled that makes it evident that this is absolutely not about public health.
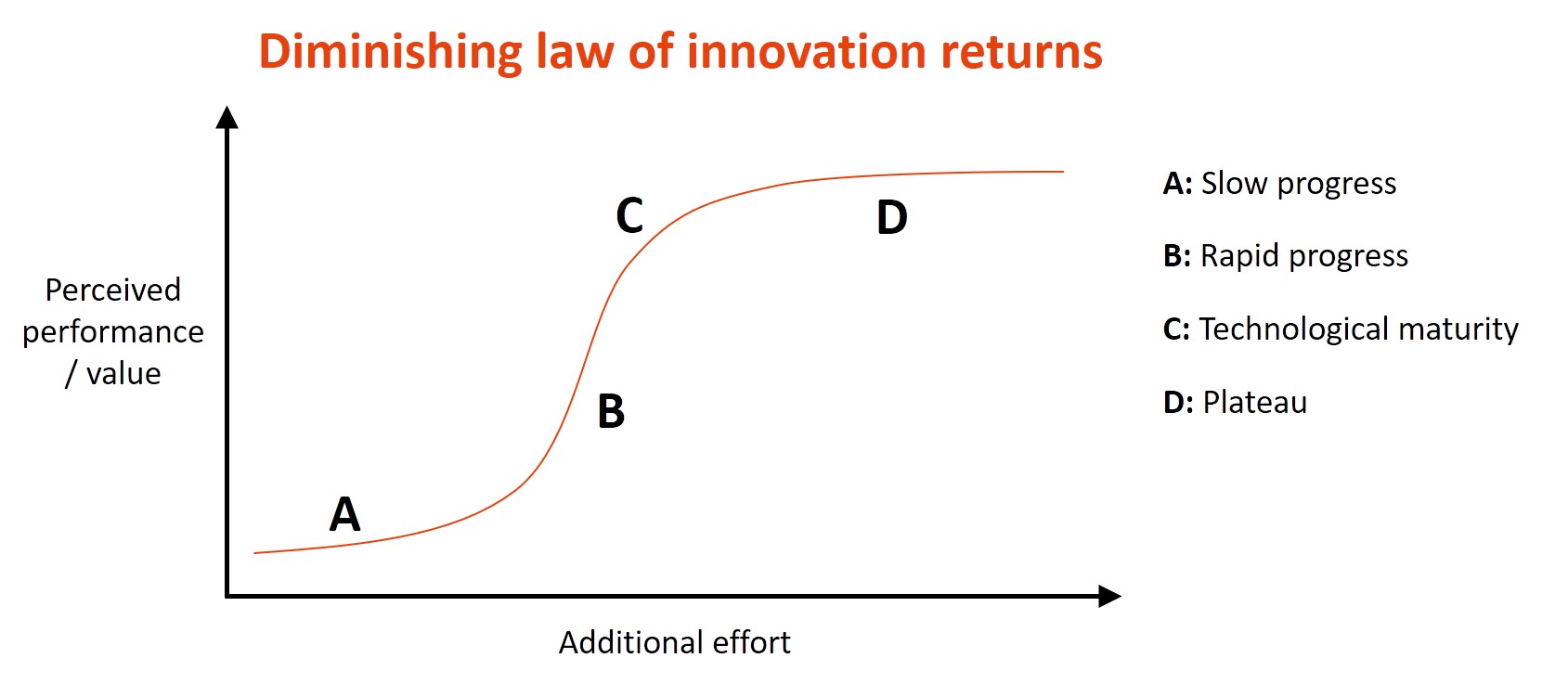
Consider the typical diminishing returns curve in complex systems. Imagine a simplified diminishing returns curve where the x-axis is investment. The y-axis is return. There is a shallow early phase that then curves up and becomes a steep, effectively a cliff face, in which your investment is low relative to the returns that you get for it. For example, in the early stages imagine you are trying to figure out how to skateboard, or whatever it may be, and it’s tough at first and then you hit some point where you are, like, “Oh, I’m getting this, I’m getting this!” And then what happens? At the inflection point in the curve you get the emergence of a plateau, where larger and larger investments net smaller and smaller gains. There are still returns on investment, but they get less and less.
The reason that you get a diminishing returns curve in a complex system in which there’s an objective, is that you have a hierarchy of interventions. You’ve got some stuff that’s actually “no-brainers” that work really well, and you do those things first. This is obvious, of course, because why wouldn’t you? The more of those “most evident” things you’ve already done, the more of the low-hanging fruit you’ve found, the more you’re forced to do things that, yes, work. But at increasingly larger costs. And so you get this reliable pattern because a reasonable person, or system, attempting to solve a problem will go after the low-hanging fruit first. Eventually you will be left with smaller and smaller interventions that are more and more expensive, eventually getting to a point of near pointlessness.
Our response to COVID does not show an indication that we have gone after the low-hanging fruit. At all. It’s completely insane with respect to the low-hanging fruit that we have left on the table and not invoked. For instance, the most obvious one, and the thing that I would suggest that we use as a litmus test, is the question of vitamin D. Now the vitamin D question is not simple. It’s not a simple matter of, take vitamin D = avoid COVID. You can take vitamin D and still get COVID. But the evidence strongly suggests that vitamin D deficiency makes you much more vulnerable to COVID. This is completely unambiguous. And what’s more, that people who live far from the equator, as many of us do, are very likely to be vitamin D deficient during the winter months. Why? Because vitamin D is naturally produced on the skin in response to sunlight, and so what that means is that vitamin D deficiency, which might not be inherent to humans, is very common amongst modern humans because of the way we live. Because we spend a lot of time indoors where climate control allows us to continue, but we are then chronically underexposed to sunlight that would produce vitamin D. And therefore vitamin D supplementation has tremendous value in terms of fending off COVID for people who are likely to experience deficiencies. What’s more, vitamin D is inexpensive, vitamin D is readily available, and not only does vitamin D not have serious downsides, but if you take reasonable amounts of vitamin D you are very likely to fend off other diseases because vitamin D is basically immunosuppressive. All this makes a great deal of sense, and yet we are somehow still not widely recommending vitamin D to everybody who are likely to have that deficiency in the winter. In spite of the fact that we have a raging pandemic and we could reduce the number of cases substantially by simply making that one intervention.
So the question is, how on earth is this not our first public health recommendation to people? That if you have any danger of a vitamin D deficiency, you should do something about it. That includes making vitamin D while the sun shines – by going outside and exposing yourself to sunlight. And as that becomes less and less useful as an intervention, supplementing with biologically available vitamin D that would compensate for a deficiency. I would say that’s a litmus test. Why is it a litmus test? Because it’s the lowest hanging fruit on the tree. There is no good reason not to address the question of vitamin D deficiency first. It should have been our first intervention. And the fact that we didn’t do it, and still are not doing it, is evidence of one of two things. It is either evidence of absolutely jaw-dropping levels of incompetence (which I admit is possible). Or, that something else is driving our policy that isn’t really obsessed with preventing COVID.